Tobacco Use and Skin Disease
Published: 06/01/2001
Abstract and Introduction
Abstract
Background. The primary objective of this review is to evaluate the mucocutaneous manifestations of tobacco use.
Methods. Computerized literature searches were conducted for English language articles related to skin/mucous membrane disease and use of tobacco. The primary criterion for assessing data quality and validity was the demonstration of a causal relationship between tobacco use and skin/mucous membrane disease.
Results. This review of the literature shows that a number of disorders and diseases of the skin and mucous membranes are related to tobacco use.
Conclusions. Since millions of persons use tobacco despite its well publicized relationship to increased mortality, knowledge of the mucocutaneous morbidity associated with tobacco use may help physicians in counseling their patients.
Introduction
Cigarette smoking is the largest preventable cause of death in the United States according to the Centers for Disease Control and Prevention.[1] Furthermore, it is well known that cigarette smoking contributes to an increased risk of cancer, coronary artery disease, stroke, chronic pulmonary disease, and aortic aneurysm. Approximately 1.1 billion people smoke, and smoking kills 1 in 10 adults worldwide.[2]
Fortunately, the annual prevalence of cigarette smoking among adults in the United States declined 40% between 1965 and 1990.[1] However, it has remained practically unchanged during 1990 and 1999 with current estimates of smoking prevalence among men of 28.0% and among women of 22.5%.[1] There has also been an increase in the use of smokeless tobacco between 1970 and 1987 among white men ≤34 years of age.[1]
The latency associated with many tobacco-related diseases ensures that tobacco-induced health problems will continue for many years to come. Although the association between tobacco and cardiovascular disease, pulmonary disease, and cancer is well known to health care professionals, the many skin diseases caused by tobacco use may be less recognizable. In this paper, we outline some of the direct and indirect effects of smoking and smokeless tobacco use that can be detected on dermatologic examination ( Table 1 ).
Table 1. Dermatologic Effects of Cigarette Smoking
| Direct Effects | Indirect Effects |
|---|---|
| Facial wrinkling | Poor wound healing |
| Facial gauntness | Psoriasis |
| Complexion color changes | Atherosclerotic peripheral vascular disease |
| Decreased skin moisture | Buerger's disease |
| Yellowed nails | Raynaud's disease |
| Harlequin nails | Diabetic foot disease |
| Halitosis | Oral yeast infections |
| Nicotine stomatitis | Condyloma acuminatum |
| Skin burns | Cutaneous findings in HIV and AIDS Crohn's disease, and malignancies |
Direct Effects of Cigarette Smoking
Cosmetic Effects
"Attractiveness" studies suggest that appearance is important in obtaining social advantages that improve the quality of life.[3] Furthermore, the psychologic impact of appearing older than one's chronologic age can be significant, especially with regard to self-perception.[4] Cigarette smoking can alter a person's physical appearance in some dramatic ways.
Although facial wrinkling is an inevitable part of aging, cigarette smoking can accelerate the process. Kadunce et al[5] found that cigarette smoking is an independent risk factor for the development of accelerated facial wrinkling and that the risk is dose dependent to smoking exposure. Smokers with a greater than 50 pack-year history were noted to be 4.7 times more likely to have wrinkles than nonsmokers, controlling for age, sex, skin pigmentation, and sun exposure. The risk was increased even further when subjects were exposed to both excessive sunlight and smoking. In another study, Ernster et al[6] found that the increased risk of wrinkling was equivalent to approximately 1.4 years of aging in smokers when compared with nonsmokers. In addition, Ernster et al[6] found that pack-years were positively associated with facial wrinkle scores in women aged 40 to 69 and men aged 40 to 59. Although there are vast differences in the data concerning this issue, all agree that smoking causes increases in facial wrinkling.
The typical smoker's face (Fig 1) was described by Model[7] as being distinguished by one or more of the following characteristics: facial wrinkles radiating at right angles from the upper and lower lips or corners of the eyes; a subtle gauntness of the facial features with prominence of the underlying bony contours; an atrophic, slightly pigmented gray appearance of the skin; and a plethoric, slightly orange, purple, and red complexion. Chemosis is also frequently observed in smokers' faces.
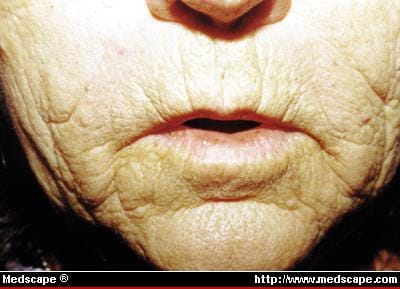
Figure 1. Smoker's facial wrinkles radiating at right angles from lips.
Several mechanisms have been proposed for the changes seen in the smoker's face. The wrinkling around the mouth and eyes could be due to repetitive facial movements such as pursing the lips to smoke cigarettes, and squinting the eyes to avoid irritating cigarette fumes. However, these mechanical factors are not widely accepted as causes for the increased wrinkling. Another factor is the increase of mean relative area, number, and thickness of the dermal elastic fibers seen in the non-sun-exposed skin of smokers, which are similar to changes seen in solar elastosis.[8] Elastotic skin is less elastic, dryer, darker, and more erythematous than normal skin,[9] which could account for some of the smoker's skin changes, especially in sun-exposed areas. Also, under investigation are changes in the microvasculature of skin exposed to cigarette smoke, which include chronic reduced blood flow to the skin.[10] This process, which includes nicotine-induced vasoconstriction, could result in premature aging. There is some evidence that premature resorption of facial bones, possibly due to an antiestrogenic effect of smoking,[11,12] could help explain the smoker's gaunt and wrinkled appearance, but these antiestrogenic effects are poorly understood and slightly controversial. Finally, several studies link smoking with significant decreases in skin moisture,[13] which also could contribute to a dry wrinkled appearance.
Another direct cosmetic effect of cigarette smoking is the yellow pigmentation of the fingernail plate, commonly referred to as the "nicotine sign" (Fig 2). Tobacco by-products from cigarette smoke actually stain the nails. Verghese et al[14] described another nail sign that occurs when a long-time smoker suddenly ceases smoking due to illness (commonly a stroke). A distinct line of demarcation is seen between the distal, yellowed nail and the newly grown proximal nonpigmented nail. This sign is termed "harlequin nail." According to the authors, the date a patient has ceased smoking can be deduced by measuring the distance between the nail base and the line of demarcation. This could be a useful tool when patients are unable to volunteer information about the onset of illnesses.

Figure 2. "Nicotine sign"--yellow pigmentation of fingernail plate and sclerodactyly in a man with 100 pack-year history of cigarette smoking.
Nicotine Stomatitis
Nicotine stomatitis, otherwise known as smoker's palate or leukokeratosis nicotine palati, is an asymptomatic stomatitis usually seen in chronic smokers. It is described as an inflamed, reddened mucosa that progresses to a multinodular, papular, gray-white keratinized mucosa[15] and usually only involves the palate. The papules are inflamed and sometimes plugged salivary glands. The red central spot represents the salivary duct orifice.
Burns
An important and often unappreciated health effect of smoking is the cigarette-initiated fire. Cigarettes are, by far, the leading cause of deaths from residential fires.[16] In an epidemiologic study of fires, cigarettes were determined to be the ignition source of 55% of fatal fires investigated.[17] The odds ratio for fire injury in households where members collectively smoked 1 to 9 cigarettes per day was 1.5 compared with households with no smokers; for 10 to 19 and more than 20 cigarettes per day the ratio was 6.6 and 3.6, respectively.[18] The resulting burns can range from minor superficial thermal injury to severe, extensive skin loss, and death. In addition, the resulting scars have an increased rate of squamous cell carcinoma.[19]
Indirect Effects of Cigarette Smoking
Atopic Dermatitis
Although previous studies have linked childhood dermatitis with maternal smoking, recently Mills et al[20] reported no apparent difference in the prevalence of atopic dermatitis in smokers or control patients.
Psoriasis
Many researchers have shown a relationship between smoking and psoriasis, especially palmopustular psoriasis. O'Doherty et al[21] showed that palmopustular psoriasis was associated with a high prevalence of smoking. In addition, Mills et al[22] showed that in plaque psoriasis, there was a significantly higher prevalence of current smoking (46%) as compared with matched controls (24%), and more patients with psoriasis had smoked before the onset of psoriasis (55%) as compared with controls (32%). Finally, the daily consumption of cigarettes correlated with the risk of developing psoriasis, with the higher number of cigarettes smoked (more than 20 cigarettes per day) being associated with greater risk. This was confirmed by Poikolainen et al,[23] who found that among psoriatic women the mean number of cigarettes smoked was 8.6 compared with 4.7 for controls. It should be noted that some treatments for psoriasis are flammable and therefore may pose a danger to smokers.
Crohn's Disease
Cigarette smoking has been recognized as a risk factor in Crohn's disease. Relative risk for ever-smokers versus never-smokers is 4.0, and the risk increases with the number of cigarettes smoked and the duration of the habit.[24] A retrospective study from the University of Calgary in Alberta further shows that cigarette smoking strongly influences disease activity after surgery.[25] The recurrence rate 10 years after surgery for Crohn's disease was 70% for smokers and 41% for nonsmokers. In comparison, the risk of ulcerative colitis appears to decrease in smokers and increase in former smokers.[26]
Cutaneous lesions develop in up to 15% of patients with Crohn's disease.[27] Although more common in ulcerative colitis, pyoderma gangrenosum has been shown to occur in approximately 1.2% of patients with Crohn's disease.[28] Ulceration, fistula formation, and cutaneous abscesses of the perineum are common in patients with Crohn's disease.[29] A persistent fistula may, in fact, be the presenting complaint in Crohn's disease.
Aphthous ulcers, often intractable, are seen in up to 9% of patients with Crohn's disease and are the most common oral manifestation of the disease.[30] (However, smokers have been shown to have fewer aphthous ulcers than nonsmokers.[31]) Other oral manifestations include gingival or buccal cobblestoning, scarring, and elongated ulcers and nodules.
Granulomas occur in Crohn's disease around the anus and at scar, fistula, and colostomy sites. A relatively rare dermatologic manifestation is termed metastatic Crohn's disease, in which granulomatous cutaneous lesions are found in areas remote from the gastrointestinal tract.[32] These lesions can appear as erythematous plaques, nodules, or ulcers and usually involve the lower extremities.
Other cutaneous manifestations of Crohn's disease include erythema nodosum, necrotizing vasculitis, nutritional changes, finger clubbing, and palmar erythema.[33] An association between Crohn's disease and psoriasis has been found. The frequency of psoriasis in patients with Crohn's disease is 7.6 times the normal rate.[34] Vitiligo has also been noted in patients with Crohn's disease, though the association may merely represent a chance occurrence.[35]
One report describes an unusual cutaneous manifestation of Crohn's disease involving an erythematous malar plaque that followed the clinical course of the bowel disease but was not granulomatous.[36] Histologically, the lesion was described as an "atypical Sweet's-like eruption with giant cells." The lesion possibly represents a previously unrecognized pattern of Crohn's disease affecting the skin.
Nutrition
Aside from nutritional deficiencies that can arise in patients with Crohn's disease, cigarettes have some effects on the nutritional status of smokers. In the United States, the second National Health and Nutrition Examination Survey (NHANES II) of 1976 to 1980, showed that serum vitamin C levels were lower in smokers for each level of dietary vitamin C intake.[37] An analysis of the data from the NHANES II confirms the association between smoking and decreased serum vitamin C levels, even while correcting for other factors that also affect vitamin C levels such as age, sex, race, and body mass index.[38] The risk of severe hypovitaminosis C (<0.2>
The serum level of vitamin C sufficiently low to produce clinical signs of scurvy is not well defined, but levels in reported cases have been 0.4 mg/dL or less.[39] The dermatologic manifestations of deficient vitamin C status include follicular hyperkeratosis, "corkscrew" hairs, and perifollicular and closed space hemorrhages.[40] Oral manifestations include gingival hypertrophy with friable gums. Another particularly important result of hypovitaminosis C is poor wound healing. In the absence of vitamin C, in fact, an eightfold increase in wound dehiscence has been shown to occur.[41] Therefore, lower vitamin C levels may contribute to the healing problems seen in smokers.
Response to Antimalarials
Cigarette smoking interferes with the effectiveness of antimalarial therapy for cutaneous lupus erythematosus. One report showed a significant difference (P < .0002) in the antimalarial response rate between smokers (40%) and nonsmokers (90%) in a group of 61 patients with lupus erythematosus.[42]
Acne
As with aphthous ulcers, smoking or some component of cigarette smoke may have a protective effect against the development of acne. Mills et al[43] interviewed 165 patients with acne (96 male and 69 female) and compared these individuals' smoking habits to national statistics. Only 19.7% of the male subjects and 12.1% of the female subjects were smokers, which is much lower than the expected national prevalence of 34.5% and 32.7%, respectively. The findings support the hypothesis that some component of cigarette smoke, possibly nicotine, has an anti-inflammatory action on acne. Another factor may be that patients who seek treatment for acne are more attuned to health issues and are less likely to smoke. Whatever the reason may be, physicians would not be willing to encourage acne sufferers to smoke just to improve this non-life-threatening disorder. This study looked only at patients with serious acne and the results may not apply to patients with moderate acne.
Healing
An important consideration in dermatologic operations (especially cutaneous flaps) is the effect that smoking has on healing. Evidence suggests that cigarette smoking can impede healing. Patients who smoked before and after face lifts showed a statistically greater incidence of wound slough than nonsmokers.[44] Smoking also has been associated with a decreased healing rate after surgical removal of impacted teeth,[45] and chronic smoking was shown to adversely affect periodontal healing after surgery for periodontitis.[46] Rugg et al[47] observed that patients who smoked during radiotherapy for head and neck cancers (which are commonly caused by smoking) took 21 weeks to heal the resulting mucositis, compared with 13 weeks in those not smoking during treatment. Mosely and Finseth[48] described a patient with a nonspecific arteritis whose fingertip ulcer would not heal for 5 months until smoking was discontinued. Goldminz and Bennett[49] showed that high-level smokers (defined as ≥1 pack per day) had necrosis of flaps and full-thickness grafts at approximately three times the rate of never smokers, low-level smokers, or former smokers. Also, once tissue necrosis had developed, the median percentage of the visibly necrosed flap or graft tissue was threefold greater among current smokers (regardless of number of packs smoked per day) than never smokers.
Animal experiments confirm the results of the clinical investigations. Nolan et al[50] found that skin flaps on rats exposed to cigarette smoke after surgery showed a significantly greater mean percent area of flap necrosis compared with sham-exposed groups or control groups not exposed. Lawrence et al[51] found that 75.2% of flaps in the control rats survived for 7 days, compared with 48.1% in the rats exposed to intermittent cigarette smoke. Blood gas values in the smoke-exposed rats showed an elevation of carboxyhemoglobin similar to that in human smokers. Rees[52] also found that hamsters exposed to cigarette smoke before and after flap surgery showed a significant increase in flap necrosis.
Cigarette smoking has been shown to reduce blood flow, especially to the extremities. Using the ultrasonic Doppler flow meter, Sarin et al[53] concluded that smoking a single cigarette reduced mean blood flow velocity by 42% in the digital vessels of male volunteers. Mosely and Finseth[48] showed via angiogram that smoking a single cigarette produced severe vasoconstriction in a patient.
The two constituents of cigarette smoke that have been studied and appear to affect healing and flap survival are nicotine and carbon monoxide. Several well-known effects of these constituents are described. Nicotine stimulates the sympathetic ganglia, causing peripheral vasoconstriction. Nicotine also stimulates chemoreceptors of the carotid and aortic body and causes release of catecholamines and further vasoconstriction.[50] These catecholamines also act as cofactors in the formation of chalones, which in turn inhibit epithelialization.[54]
Carbon monoxide binds with great affinity to hemoglobin, reducing the amount of oxygen carried. Because of the shift to the left in the oxyhemoglobin dissociation curve, oxygen that is carried is not released effectively to tissues. Carbon monoxide also increases platelet adhesiveness,[55] and the increase in carboxyhemoglobin seen in smokers has been shown to induce significant endothelial changes.[56]
Reduction of blood flow due to nicotine effects and impairment of oxygenation due to the carbon monoxide could impair the healing process.[48] Certainly, other mechanisms by which tobacco impairs healing exist, but they have been less thoroughly studied thus far.
Because of overwhelming evidence of the effects of cigarette smoking on healing, it is advised that patients refrain from smoking at least 12 waking hours before surgery, since it takes that long to clear carbon monoxide and bring carboxyhemoglobin levels to near normal.[57] Furthermore, smoking abstinence should be continued during the immediate postoperative period to prevent a "wound disaster."[53]
Atherosclerotic Peripheral Vascular Disease
Cigarette smoking is the most powerful risk factor for atherosclerotic peripheral vascular disease, and smoking cessation is the most important intervention in managing the problem.[58] In one study, pack-years of cigarettes smoked was found to be strongly associated with large vessel peripheral arterial disease.[59] Diabetics who smoke cigarettes have the highest risk for lower extremity arterial disease and amputation.[58] Lithner[60] reported that practically all diabetics less than 60 years old who had gangrene were cigarette smokers, and those diabetics who stopped smoking for at least 2 years had a 30% lower prevalence of lower extremity arterial disease than those who continued smoking.
A strong association between cigarette smoking and development of diabetic neuropathy in patients with insulin-dependent (type I) diabetes has also been observed.[61] A dose-response relationship was found between lifetime cigarette smoking and neuropathy. Patients with ≥30 pack-year histories of smoking were 3.32 times more likely to have neuropathy than patients smoking less than this amount. The mechanism proposed for this effect is that tissue hypoxia produced by cigarette smoking results in injury to the neural microvasculature. Peripheral neuropathy can render the diabetic's foot insensitive to the presence of an ulceration, leading to delayed treatment and potentially disastrous sequelae.[61]
The major clinical manifestations of peripheral vascular disease are those of ischemia. Intermittent claudication may be accompanied by muscle atrophy of the foot, calf, or thigh. Examination of the foot in peripheral vascular disease reveals several typical dermatologic findings.[62] The foot is cold to the touch, and the skin is shiny, dry, and atrophic. No hair will be present on the feet or toes. Fat pads of the heel and toes may atrophy. Color depends on position: it may show blanching with elevation and cyanotic redness with dependency. With severe ischemia, the skin ulcerates, usually starting at the tips of the digits. These painful ulcers are shallow, with a sloughing dark base. A characteristic necrotic crack may form on the heel, which gradually ulcerates. Nail growth is slowed; cracking of the nail plate and pterygium formation may occur.[63]
Atheromatous emboli may also cause multiple, small ulcers. These can cause recurrent episodes of painful blue toes, petechiae, or livedo reticularis.[62]
Thromboangiitis Obliterans
Thromboangiitis obliterans (Buerger's disease) (Fig 3) is an obstructive vascular disease caused by segmental inflammatory and proliferative lesions of the tunica media of small arteries and veins.[64] The cause is unknown, but the disease is strongly associated with smoking. Almost all patients with this disease have a history of heavy cigarette smoking, and cessation and resumption of smoking have been documented to produce remission and exacerbation of the disease.[65] A case has been reported relating smokeless tobacco use to Buerger's disease as well.[66] It appears that some constituent in tobacco, whether smoked or chewed, acts as a cofactor in the development of the disease.

Figure 3. Thromboangiitis obliterans (Buerger's disease) of large toe in smoker.
An autoimmune mechanism is suggested in Buerger's disease by a study in which approximately 50% of patients had significant levels of anticollagen antibodies in their blood, and 77% of patients exhibited cellular sensitivity to human type I and type II collagen.[67] A genetic predisposition also appears to be present, since patients with the disease have a high prevalence of HLA-A9 and HLA-B5 antigens.[68]
This disease occurs predominantly in young men and usually affects the lower extremities and, less often, the upper extremities. Occasionally, visceral arteries are involved such as coronary, cerebral, renal, or mesenteric arteries. In addition, the first case of Buerger's disease involving orofacial vessels has been reported.[65]
Physical examination in Buerger's disease reveals impaired distal pulses in the affected limb such as the radial, ulnar, dorsalis pedis, and posterior tibial pulses.[64] Palpation of proximal pulses, however, is normal. Manifestations of distal limb ischemia include cyanosis, pallor, or persistent erythema with an associated change in temperature. Postural changes in color are noted, as are ulcerations or localized gangrene of the digits. Edema of the foot is common. Intermittent claudication in the lower extremities occurs, especially in the arch of the foot. Cold sensitivity with paresthesias and development of secondary Raynaud's phenomenon are common. Superficial thrombophlebitis can be migratory and is manifested as tender, red, inflamed segments of superficial veins.
Raynaud's Syndrome
Digital ischemia caused by either vasospasm or obstruction causes the typical Raynaud's episode. This syndrome, seen more often in women, usually involves the hands and fingers, and often is a response to cold temperature or other stimuli.
The usual attack begins with blanched digits, due to cessation of arterial blood flow, followed by cynanosis on rewarming. Later, erythema occurs, caused by reactive hyperemia.
The vasospastic episodes are generally induced by cold temperature, but can be induced by nicotine or caffeine use. Alternatively, the obstructive episodes are most often due to an underlying disease process such as atherosclerosis, trauma, connective tissue disorder, or Buerger's disease. It is obvious that cigarette smoking can aggravate and initiate this condition directly by causing vasospasm and indirectly by involvement in some obstructive diseases.
Cigarette smoking may have a role in irreversible tissue injury sometimes found in Raynaud's syndrome. One study suggests that ascorbic acid and selenium deficiencies may predispose toward irreversible tissue damage in these patients.[69] As previously mentioned, ascorbic acid deficiency is known to occur in smokers.
Cancer
The 1989 Surgeon General's Report concluded that cigarette smoking causes lung cancer, laryngeal cancer, oral cancer, and esophageal cancer. Furthermore, recent studies have established that passive smokers also have an increased risk of lung cancer.[70,71] The 1989 Surgeon General's Report[58] also recognized cigarette smoking to be a contributing factor in cancer of the bladder, pancreas, lip (Fig 4), and kidney and to be associated with cancer of the stomach and uterine cervix. The estimated contribution of cigarette smoking to all cancer deaths is 30%.[58] The cutaneous manifestations of the many cancers associated with cigarette smoking are too numerous to cover completely, but some of the most interesting are described in Table 2 .
Table 2. Dermatologic Findings in Smoking-Related Malignancies
| Dermatologic Findings | Related Malignancy |
|---|---|
| Skin metastases | All smoking related malignancies |
| Clubbed nails | Bronchogenic carcinoma |
| Raynaud's syndrome | Pancreatic or lung carcinoma |
| Acute febrile neutrophilic dermatosis | Acute myelogenous leukemia |
| Leonine facies | Myelogenous leukemias |
| Leukocytoclastic vasculitis | Bronchogenic carcinoma |
| Migratory superficial thrombophlebitis | Pancreatic or lung carcinoma |
| Acquired ichthyosis | Cervical or lung carcinoma |
| Erythroderma | Hematologic malignancies |
| Generalized pruritus | Pancreatic carcinoma |
| Acrokeratosis paraneoplastica | Carcinoma of esophagus, lip, tongue, pharynx-larynx, or upper third of lung |
| Erythema gyratum repens | Lung carcinoma |
| Subcutaneous fat necrosis | Pancreatic carcinoma |
| Gynecomastia | Lung carcinoma |
| Hypertrichosis lanuginosa acquisita | Pancreatic or lung carcinoma |
| Multiple eruptive seborrheic keratoses | Lung carcinoma |
| Cushing's features | Lung carcinoma (small cell) |

Figure 4. Squamous cell carcinoma of lip in pipe smoker.
Skin metastases occur in 0.7% to 9.0% of all patients with cancer.[72] In fact, skin metastases can be the first sign of visceral cancer; in one study, they were the presenting sign in 3.7% of men and in 6% of women.[73] All of the cancers associated with cigarette smoking have been known to metastasize to the skin. Metastatic spread from a distant primary tumor to the skin can be one aspect of diffuse metastatic disease or can be the first sign of malignancy in an otherwise asymptomatic patient.[74] As a general rule, in tumors that metastasize via the lymphatics, such as squamous cell carcinoma of the oral cavity and transitional cell carcinoma of the bladder, skin metastases appear late in the course of the disease and frequently appear in the skin overlying the primary lesion. Tumors that metastasize hematogenously, such as carcinoma of the kidney and lung, often first present cutaneous metastases in an otherwise asymptomatic patient and appear in the skin at distant sites from the primary (Fig 5).

Figure 5. Cutaneous metastasis as presenting sign of squamous cell carcinoma of lung in smoker.
Paraneoplastic syndromes frequently produce dermatologic effects. Lung cancer, especially small cell lung carcinoma, is the most common tumor causing ectopic ACTH production.[75] Classic features include generalized hyperpigmentation, cutaneous striae, centripetal obesity, buffalo hump, and moon facies. This syndrome is only rarely the presenting sign of underlying malignancy, but these signs are useful in determining the success of treatment. Carcinoma of the lung has also been known to elaborate gonadotropins, producing painful gynecomastia.[76]
Paraneoplastic acrokeratosis (Bazex syndrome) has been associated with many cancers caused by tobacco use, including neoplasia of the lower lip, tongue, esophagus, pharyngolaryngeal region, and upper third of the lung. Skin changes are characterized by violaceous erythema with a slight psoriasiform scaling that first appears on the fingers and toes. The nails frequently become hypertrophic with onycholysis during the initial stages. Next, a pityriasiform scaling and violaceous erythema develop on the aural helices and nose. Eventually, all surfaces of the hands and feet may become involved, and psoriasiform lesions may develop on the legs, arms, scalp, and face.[77] These skin lesions usually precede symptoms of the underlying malignancy, so an extensive examination is warranted if they are observed.
Present evidence strongly suggests an association between cigarette smoking and leukemia. A large prospective study has shown a significant increase in the risk of leukemia, especially acute nonlymphocytic leukemia.[78] This study further shows a dose-response relationship between cigarettes smoked and risk. An additional recent case-control study showed that smokers had a twofold increased risk of acute, nonlymphocytic leukemia compared with nonsmokers.[79] Another study showed the risks of leukemia and myeloma increase with duration of smoking.[80] Whether the association between leukemia and cigarette smoking represents a cause-and-effect relationship remains to be seen, and a mechanism is yet to be identified.[81]
The myeloid leukemias infiltrate the skin more frequently than other leukemias. They usually are manifested as papules or nodules from 1 to 20 mm in diameter and vary in color from normal skin tone to deep purple. The trunk is usually involved with relative sparing of the face, scalp, and extremities.[82] These lesions can produce a leonine facies as well.[83] Although skin involvement usually develops well after the diagnosis of leukemia, it can at times be the first manifestation, often months before peripheral blood involvement.[82] Another point to be made is the difficulty in diagnosing the skin infiltrations in leukemia. Monoclonal antibodies for myeloid cells must be included in the diagnostic panel of skin biopsies.[84]
Acute myelogenous leukemia is the most common malignancy to be associated with acute febrile neutrophilic dermatosis (Sweet's syndrome).[85] Cutaneous manifestations of the leukemias are varied, and additional skin findings include hemorrhagic lesions, generalized pruritus, exfoliative erythroderma, pyoderma gangrenosum, urticaria, erythema multiforme, erythema nodosum, panniculitis, hyperpigmentation, and morbilliform eruptions.[84]
One case is reported of a patient with follicular mucinosis and mycosis fungoides. One week after this diagnosis, myeloblasts were seen in the peripheral blood.[86]
Although cutaneous metastases from transitional cell bladder cancer have been considered rare, Spector et al[87] reported three cases in a 3-year period from their community hospital, with an average incidence of bladder cancer. They suggested that the apparent increased occurrence they had reflects added longevity in patients who have been successfully treated. These metastases usually present themselves as multiple firm, red, fixed papules and nodules.[88] They usually appear metachronously long after the primary bladder lesion has been diagnosed, at a time when multiple organ metastases have occurred.
Acquired ichthyosis has been associated with lung and cervical cancer.[89] Cutaneous changes are usually noted after the primary disease is diagnosed. Parallel fluctuations in the malignancy and the skin disorder suggest that this dermatosis may be useful in monitoring the course of the underlying malignancy. It is manifested by generalized dry skin and pruritus, and generalized scaling is seen on physical examination. Ichthyosis, unlike xerosis, will not respond to topical emollients.
Erythroderma, which presents as a diffuse erythema, induration, and scaling of the skin, is usually associated with hematologic malignancies.[90] In patients with carcinoma of the lung or pancreas, erythroderma usually occurs in the later stages of disease.
Vascular abnormalities can signal an internal malignancy as well. Leukocytoclastic vasculitis can be a presenting sign in squamous cell carcinoma of the bronchus.[91] Digital ischemia manifested as Raynaud's phenomenon or gangrene may be a marker for carcinoma of the pancreas or kidney.[92] Migratory superficial thrombophlebitis is strongly associated with lung, pancreas, and gastric carcinomas, and is probably related to a hypercoagulable state.
When a patient has dermatomyositis, a directed search for malignancy is justified, including thorough history, physical examination, and screening laboratory tests followed by workup of any abnormality found.[93] The reported frequency of cancer in dermatomyositis is variable, ranging anywhere from 10% to more than 50%.[94] Two recent studies reported that 41%[95] and 43%[94] of patients with dermatomyositis had an associated malignancy. The frequency of tumor types is similar to that found in the general population.[93] The cutaneous manifestations of dermatomyositis include a purplish-red periorbital discoloration, or heliotrope rash, which is prominent on the upper eyelids. The dermatitis is erythematous, scaly, macular and papular, involving the forehead, malar area, neck, and extensor surfaces of the extremities. Poikiloderma, areas of atrophy, vitiligo, or hyperpigmentation, may develop from the original cutaneous lesions. Erythema and infarction of dilated capillaries at the nail margins are common as well.[96]
Generalized pruritus, along with the lesions induced by the subsequent rubbing or scratching, is only rarely associated with malignancy, but it has been seen with pancreatic tumors.[97]
Erythema gyratum repens (Fig 6) is almost always associated with an underlying neoplasm, most commonly of the lung. It has also been seen in association with carcinomas of the cervix, bladder, tongue, and hypopharynx. It presents as concentric, raised, erythematous bands that advance rapidly over the skin in a "woodgrain" pattern.[98]

Figure 6. Erythema gyratum repens as presenting sign of squamous cell carcinoma of lung in smoker.
Subcutaneous fat necrosis can be seen in acinar cell carcinoma of the pancreas. The lesions are painful subcutaneous nodules that are skin colored to violaceous, and normally occur over the trunk, buttocks, and legs.[91]
Hypertrichosis lanuginosa acquisita has been reported in association with tumors of the lung[99] and pancreas.[100] Multiple eruptive seborrheic keratoses (the sign of Leser-Trélat) have been associated with lung carcinomas.[101]
Karagas et al[102] studied patients with previous nonmelanoma cancer and found that these individuals had an increased risk for a new tumor of the same histologic type. They also found that those individuals with previous squamous cell carcinoma of the skin had an even greater risk of having another similar tumor if they smoked cigarettes. Compared with those who had never smoked, the rate of subsequent squamous cell skin cancer was higher among current smokers (rate ratio, 2.01) and former smokers (rate ratio 1.62) and increased with both duration and amount smoked.
The nails can provide clues to internal malignancies caused by cigarette smoking. Clubbed nails, or hippocratic nails, are frequently associated with malignant bronchopulmonary disease. Clubbing develops in 5% to 12% of patients with bronchogenic carcinoma.[83] This nail sign develops as a fibrovascular network that forms between the nail matrix and bone, subsequently elevating the matrix.[103] Lovibond's angle, an angle >180°, is created between the proximal nail fold and the nail plate. This syndrome can progress to hypertrophic pulmonary osteoarthropathy, in which the clubbing is accompanied by painful periostitis of the long bones and occasionally polyarthritis.[75]
Another nail deformity that has been associated with malignancy is the yellow nail syndrome. Although the association has not been proven, a case has been reported of yellow nail syndrome and concurrent squamous cell carcinoma of the bronchus.[104] In a reported case of carcinoma of the larynx and yellow nail syndrome, the patient's nails regrew normally after laryngectomy.[105] Yellow nail syndrome, in contrast to the previously mentioned yellowish staining of nails by tobacco byproducts, is characterized by a striking yellow to green color, and is accompanied by other nail findings in addition to the coloration. The nails are thickened and have transverse ridging, as well as increased transverse curvature with formation of a hump. They also have slowed growth, absent lunulae and cuticles, and onycholysis.[106]
Human Papillomavirus
Cigarette smoking appears to be associated with several infectious processes that can be discovered upon dermatologic examination. Heavy cigarette smoking is a predisposing factor for development of oral yeast infections.[107] Cigarette smoking has been associated with condyloma acuminatum as well.[108,109]
Daling et al[108] found that in women who had ever smoked, the risk of condyloma was 3.7 times that of women who had never smoked. Adjustment was made for factors such as number of sexual partners, history of other sexually transmitted diseases, and duration of oral contraceptive use. In women who smoked for 3 years or more, the relative risk of condyloma rose to 4.3. One possible factor in the development of condyloma in smokers is that nicotine appears to have a toxic effect on the epithelium, which may facilitate the entry of human papilloma virus.[109] Another possible explanation for an increase of such infections in smokers is the effect that smoking has on the immune response. Leukocytes from cigarette smokers have reduced natural killing capacity compared with leukocytes from nonsmokers.[110]
Human Immunodeficiency Virus
Dermatologic disease is a common occurrence in the individual infected with the human immunodeficiency virus (HIV). These patients have an increased risk for development of many cutaneous disorders, including Kaposi's sarcoma, eosinophilic folliculitis, psoriasis, molluscum contagiosum, seborrheic dermatitis, candidiasis, oral hairy leukoplakia, genital warts, genital herpes, and herpes zoster.
Although cigarette smoking has long been known to affect CD4 lymphocytes in immunocompetent individuals,[111] recent studies reveal that smoking plays a role in HIV infection and acquired immunodeficiency syndrome (AIDS). Evidence indicates that cigarette smoking may affect the immune system response to HIV-1 infection and natural progression of the disease.
Patients with AIDS who smoked were found to be more likely to have HIV-1 infiltration of the lung. This condition can often be detected in patients having respiratory episodes and is associated with a more rapid progression to death.[112] Another study found that in HIV-1 infected individuals who smoked, Pneumocyctis carinii pneumonia (PCP), an AIDS-defining diagnosis, developed more rapidly than in nonsmokers, with a median time to PCP of 9 months, compared with 16 months for nonsmokers.[113]
Burns et al[114] assessed AIDS risk in 202 homosexual men and found that among subjects who were initially seronegative, smokers were more likely than nonsmokers to become HIV-1 seropositive. Data reveal not only that smoking may be a marker for high-risk behavior in homosexual men, but also that smoking may alter the immune system, thus allowing infection.
Finally, HIV-1 seropositive individuals who smoke seem to have a reduced progression time to AIDS. Neiman et al[113] found that progression time of HIV-1 infection to the development of AIDS was 8.17 months in smokers and 14.5 months in nonsmokers. This trend is probably related to the increased number of respiratory problems seen in HIV-1 infected individuals who smoke, and these patients should be strongly encouraged to quit.
Smokeless Tobacco
Use of smokeless tobacco, including snuff and chewing tobacco, was introduced to the United States by colonists in the 17th century, and the practice remained popular throughout the 18th and 19th centuries. In the late 1800s, leaders in medicine, such as Pasteur and Lister, associated the habit with germs and communicable disease transmission, and the practice of chewing and spitting gradually became supplanted by cigarette smoking.[115] Since the 1970s, the trend has reversed. Between 1970 and 1980, the increase in sales of smokeless tobacco was estimated at 11% per year,[116] with an estimated total of 12 million American users in 1985.[117] In the early 1970s, the majority of users were men over the age of 50,[118] but more recently, in 1987 and 1991, use was most prevalent among white men aged 18 to 24. These facts are cause for concern, because the increase in use and the decrease in age at start of habit formation could lead to increasing incidences in the cancers associated with smokeless tobacco.
Cancer
The association between smokeless tobacco and cancer was noted back in 1761 by a British physician whose patients had "nasal polypuses" that he attributed to the use of dry snuff nasally.[119] Since the early 1800s, reports have described mouth cancers in those using tobacco orally.
In a key study of women in North Carolina, Winn et al[120] showed that the risk of oral cancer in nonsmokers was 4.2 times greater for those who used snuff than those who did not. Those women who used snuff for 50 years or longer were 48 times more likely to have cancer of the gum and buccal mucosa than were nonusers. In this study, the cancers were more likely to occur in those locations of the mouth where the snuff was placed; the risk grew with increasing duration of snuff use; and factors such as diet, dental hygiene, alcohol intake, and cigarette smoking were found not to be responsible for the association. The Advisory Committee to the Surgeon General concluded from this and other case-control studies that the relationship between oral cancer and smokeless tobacco is causal.[117]
The carcinogenic effects of smokeless tobacco ( Table 3 ) are not limited to the mucous membranes of the oral cavity, as illustrated in the case of a 58-year-old man who placed snuff in his left ear for several hours daily to weekly over a period of 40 years. Upon examination for complaints of burning and tingling in the left ear, a 3 x 4 cm squamous cell carcinoma was found at the upper part of the left ear along with particles of snuff in the left auditory canal.[121] Similarly, in areas of the world where snuff is inhaled and the tobacco comes in direct contact with the nasal cavity, high rates of nasal cancer have been reported.[122]
Table 3. Dermatologic Effects of Smokeless Tobacco
| Direct Effects | Indirect Effects |
|---|---|
| Localized gingival recession | Oral carcinoma |
| Increased dental caries | Esophageal carcinoma |
| Halitosis | Pharyngolaryngeal carcinomas |
| Tooth discoloration | Gastric carcinoma |
| Tooth abrasions | |
| Oral leukoplakia |
Other tissues that come in contact with constituents of smokeless tobacco in a diluted form include the esophagus, larynx (Fig 7), and stomach, and studies of cancers at these sites show an association with smokeless tobacco use.[117] Other cancers and their associations with smokeless tobacco use have been studied, but results at this time are inconclusive.

Figure 7. Squamous cell carcinoma of pyriform sinus with direct extension to skin in smokeless tobacco user.
Leukoplakia
Smokeless tobacco can cause oral leukoplakia (Fig 8).[117] In a study of 1,109 professional baseball players, leukoplakia and erythroplakia were strongly associated with smokeless tobacco use. Of the current users, 46.3% had leukoplakia. Risk for leukoplakia was found to be associated with amount of tobacco used, recency of use, and type and brand of snuff used. The leukoplakia lesions seemed to occur rapidly with tobacco use but often resolved quickly after cessation.[123]

Figure 8. Snuff dipper's lesion of lower lip, receding gums, and yellow teeth.
Greer and Poulson[124] formulated a classification system for grading the mucosal changes of adult smokeless tobacco users. Degree 1 is a superficial lesion with color similar to the surrounding mucosa, with slight wrinkling but no obvious thickening. Degree 2 is a superficial whitish or reddish lesion with moderate wrinkling but no obvious thickening. Degree 3 is described as a red or white lesion with intervening furrows of normal mucosal color and obvious thickening and wrinkling.
Some smokeless tobacco-induced leukoplakia lesions have been shown to undergo transformation to dysplasia[125] and have developed into carcinomas.[126] Clinically, one cannot accurately distinguish dysplastic from benign lesions, and therefore biopsy is necessary to determine whether malignant transformation has occurred.
Other Oral Manifestations
Smokeless tobacco has also been associated with a localized gingival recession and increased caries in those users with coexisting gingivitis ( Table 3 ).[127] Other effects on the oral tissues linked to smokeless tobacco use include halitosis, discoloration of the teeth, and excessive wear on the teeth due to abrasives in the tobacco.[128]
Table 3. Dermatologic Effects of Smokeless Tobacco
| Direct Effects | Indirect Effects |
|---|---|
| Localized gingival recession | Oral carcinoma |
| Increased dental caries | Esophageal carcinoma |
| Halitosis | Pharyngolaryngeal carcinomas |
| Tooth discoloration | Gastric carcinoma |
| Tooth abrasions | |
| Oral leukoplakia |
Conclusion
Recognition of dermatologic signs of tobacco use can certainly be a clue to many of the serious underlying systemic diseases associated with smoking and smokeless tobacco use. We suggest that the recognition of these dermatologic manifestations can, in addition, be used as a tool to encourage smoking cessation in patients. In a study by Curry et al,[129] the graphic picturing of health effects of smoking was rated by smokers to be an important motivational factor for smoking cessation. For many users of tobacco, however, the more immediate and visible effects of this drug such as wrinkling, yellow teeth, and bad breath may provide a more compelling stimulus for smoking cessation than the knowledge that tobacco kills.[130] The physician can point out the visible effects of tobacco use in the patient and use this to initiate a discussion on the patient's tobacco use and the associated health effects. Although education of the patient on the health effects of tobacco use is an important start, addictions, like other diseases, are not cured by a few choice words. All physicians need to follow discussions on tobacco use with recommendations on how to treat the addiction. Physicians need to be aware of the cessation techniques available and know how to choose the one most helpful to the individual.[131] This may include referral to a community smoking cessation program or treatment with physician follow-up and support via behavioral approaches or pharmacologic interventions. Physicians currently find it easier to deal with the consequences of tobacco use, such as pulmonary and cardiac disease, than to deal with the addiction.[132] It is important that physicians learn to intervene and help their patients quit using tobacco.
Key Points
- Dermatologic effects of cigarette smoking include facial wrinkling, facial gauntness, complexion color changes, decreased skin moisture, yellowed nails, harlequin nails, halitosis, nicotine stomatitis, and skin burns.
- Indirect effects of cigarette smoking include poor wound healing; psoriasis; atherosclerotic peripheral vascular disease; Buerger's disease; Raynaud's disease; diabetic foot disease; oral yeast infections; condyloma acuminatum; and cutaneous findings in HIV and AIDS, Crohn's disease, and malignancies.
- Recognition of dermatologic signs of tobacco use can be a clue to many of the serious underlying systemic diseases associated with smoking and also with use of smokeless tobacco.
- Physicians need to be aware of the cessation techniques available and know how to choose the one most helpful to an individual.
References
- Centers for Disease Control and Prevention: Tobacco use -- United States, 1990-1999. MMWR 1999; 48:986-993
- Satcher D: The framework convention on tobacco control: a report for the 52nd World Health Assembly. JAMA 1999; 282:424
- Johnson DF: Appearance and the Elderly in the Psychology of Cosmetic Treatments. New York, Praeger, 1985
- Fenske NA, Albers SE: Cosmetic modalities for aging skin: what to tell patients. Geriatrics 1990; 45:59-67
- Kadunce DP, Burt R, Gress RE, et al: Cigarette smoking as a risk factor for facial wrinkling. Ann Intern Med 1991; 114:840-844
- Ernster VL, Grady D, Miike R, et al: Facial wrinkling in men and women, by smoking. Am J Public Health 1995; 85:78-82
- Model D: Smoker's face. an underrated clinical sign? BMJ 1985; 291:1760-1762
- Frances C, Boisnic S, Hartman DJ, et al: Changes in the elastic tissue of the non-sunexposed skin of cigarette smokers. Br J Dermatol 1991; 125:43-47
- Adhoute M, DeRigal J, Marchand JP, et al: Influence of age and sun exposure on the biophysical properties of the human skin: an in vivo study. Photodermatol Photoimmunol Photomed 1992; 9:99-103
- Krupsi WC: The peripheral vascular consequences of smoking. Ann Vasc Surg 1991; 5:291-304
- Basu J, Mikhail MS, Palan PR, et al: Endogenous estradial and progesterone concentrations in smokers on oral contraceptives. Gynecol Obstet Invest 1992; 33:224-227
- Daniel M, Martiz AD, Drinkwater DT: Cigarette smoking, steroid hormones, and bone mineral density in young women. Calcif Tissue Int 1992; 50:300-305
- Wolf R, Tur E, Wolf D, et al: The effect of smoking on skin moisture and surface lipids. Int J Cosm Sci 1992; 14:83-88
- Verghese A, Krish G, Howe D, et al: The harlequin nail. a marker for smoking cessation. Chest 1990; 97:236-238
- Archard HO: Biology and pathology of the oral mucosa. Dermatology in General Medicine. New York, McGraw-Hill, 3rd Ed, 1987, pp 1193-1194
- Fire in the United States. Washington, DC, Federal Emergency Management Agency, 6th Ed, 1987
- Mierley MC, Baker SP: Fatal house fires in an urban population. JAMA 1993; 249:1466-1468
- Ballard JE, Koepsell TD, Rivara F: Association of smoking and alcohol drinking with residential fire injuries. Am J Epidemiol 1992; 135:26-34
- Treres N, Pack GT: The development of cancer in burn scars. analysis and report of thirty-four cases. Surg Gynecol Obstet 1930; 51:749
- Mills CM, Irivasravo ED, Harvey JM, et al: Cigarette smoking is not a risk facor in atopic dermatitis. Int J Dermatol 1994; 33:33-34
- O'Doherty CJ, MacIntyre C: Palmoplantar pustulosis and smoking. BMJ 1985; 291:861-864
- Mills CM, Irivastava ED, Harvey JM, et al: Smoking habits in psoriasis: a case control study. Br J Dermatol 1992; 127:18-21
- Poikolainen K, Reunala T, Karvanen J: Smoking, alcohol and life events related to psoriasis among women. Br J Dermatol 1994; 130:473-477
- Franceschi S, Panza E, LaVecchia C: Nonspecific inflammatory bowel disease and smoking. Am J Epidemiol 1987; 125:445-452
- Sutherland LR, Ramcharan S, Bryant H, et al: Effect of cigarette smoking on recurrence of Crohn's disease. Gastroenterology 1990; 98:1123-1128
- Greenstein AJ, Janowitz HD, Sachar DB: The extra-intestinal complications of Crohn's disease and ulcerative colitis: a study of 700 patients. Medicine 1976; 55:401-412
- Graham-Brown RAC, Rathbone B, Marks J: The skin and disorders of the alimentary tract. Dermatology in General Medicine. New York, McGraw-Hill, 5th Ed, 1999, p 1912
- Gitnick G: Inflammatory bowel diseases: Part II. Extraintestinal involvement and management. Am Fam Physician 1989; 39:225-233
- Pincus SH: Cutaneous diseases of the female genitalia. Dermatology in General Medicine. New York, McGraw-Hill, 3rd Ed, 1987, p 1264
- Croft CB, Wilkinson AR: Ulceration of the mouth, pharynx, and larynx in Crohn's disease of the intestine. Br J Surg 1972; 59:249-252
- Muzyka BC, Glick M: Major apthous ulcers in patients with HIV disease. Oral Surg Oral Med Oral Pathol 1994; 77:116-120
- Shum DT, Guenther L: Metastatic Crohn's disease. Arch Dermatol 1990; 126:645-648
- Burgdorf W: Cutaneous manifestations of Crohn's disease.
J Am Acad Dermatol 1981; 5:689-695 - Yates VM, Watkins MG, Kelman A: Further evidence for an association between psoriasis, Crohn's disease and ulcerative colitis. Br J Dermatol 1982; 1006:323-330
- Monroe EW: Vitiligo associated with regional enteritis. Arch Dermatol 1976; 112:833-834
- Smoller BR, Weishar M, Gray MH: An unusual cutaneous manifestation of Crohn's disease. Arch Pathol Lab Med 1990; 114:609-610
- Smith JL, Hodges RE: Serum levels of vitamin C in relation to dietary and supplemental intake of vitamin C in smokers and non-smokers. Ann N Y Acad Sci 1987; 498:144-152
- Schectman G, Byrd JC, Gruchow HW: The influence of smoking on vitamin C status in adults. Am J Public Health 1989; 79:158-162
- Reuler JB, Broudy VC, Cooney TO: Adult scurvy. JAMA 1985; 253:805-807
- Miller SJ: Nutritional deficiency and the skin. J Am Acad Dermatol 1989; 21:1-30
- Crandon JH, Landau JB, Mikal S, et al: Ascorbic acid economy in surgical patients as indicated by blood ascorbic acid levels. N Engl J Med 1958; 253:805-808
- Jewell ML, McCauliffe DP: Patients with cutaneous lupus erythematosus who smoke are less responsive to antimalarial treatment. J Am Acad Dermatol 2000; 42:983-987
- Mills CM, Peters TJ, Finlay AY: Does smoking influence acne? Clin Exp Dermatol 1993; 18:100-101
- Rees TD, Liverett DM, Guy CL: The effect of cigarette smoking on skin-flap survival in the face lift patient. Plast Reconstr Surg 1994; 73:911-915
- Sweet JB, Butler DP: The relationship of smoking to localized osteitis. J Oral Surg 1979; 37:732-735
- Preber H, Bergstrom J: Effect of cigarette smoking on periodontal healing following surgical therapy. J Clin Periodontol 1990; 17:324-328
- Rugg T, Saunders MI, Dische S: Smoking and mucosal reactions to radiotherapy. Br J Radiol 1990; 63:554-556
- Mosely LH, Finseth F: Cigarette smoking: impairment of digital blood flow and wound healing in the hand. Hand 1977; 9:97-101
- Goldminz D, Bennett R: Cigarette smoking and flap and full-thickness graft necrosis. Arch Dermatol 1991; 127:1012-1015
- Nolan J, Jenkins RA, Kurihara K, et al: The acute effects of cigarette smoke exposure in experimental skin flaps. Plast Reconstr Surg 1984; 75:550-551
- Lawrence WT, Murphy RC, Robson MC, et al: The detrimental effect of cigarette smoking on flap survival: an experimental study in the rat. Br J Plastic Surg 1984; 37:216-219
- Rees TD, Liverett DM, Guy G: The effect of cigarette smoking on skin flap survival in the facelift patient. Plast Reconstr Surg 1984; 73:991-996
- Sarin CL, Austin JC, Nickel WO: Effects of smoking on digital blood-flow velocity. JAMA 1974; 229:1327-1328
- Sherwin MA, Gastwirth CM: Detrimental effect of cigarette smoking on lower extremity wound healing. J Foot Surg 1990; 29:84-87
- Birnstingl MA, Brinson K, Chakrabarti R: The effect of short-term exposure to carbon monoxide on platelet stickiness. Br J Surg 1971; 58:837
- Astrup P, Kjeldsen K: Carbon monoxide, smoking and atherosclerosis. Med Clin North Am 1973; 58:323
- Anderson ME, Belani KG: Short-term preoperative smoking abstinence. Am Fam Physician 1990; 41:1191-1194
- US Department of Health and Human Services: Advances in knowledge of the health consequences of smoking. reducing the health consequences of smoking: 25 years of progress. a report of the Surgeon General. US Department of Health and Human Services, Public Health Service, Centers for Disease Control, Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health. DHHS Publication No. (CDC) 89-8411, 1989, pp 63-64
- Criqui MH, Browner D, Fronek A, et al: Peripheral arterial disease in large vessels is epidemiologically distinct from small vessel disease. Am J Epidemiol 1989; 129:1110-1119
- Lithner F: Is tobacco of importance for the development and progression of diabetic complications? Acta Med Scand 1983; 687:33-36
- Mitchell BD, Hawthorne VM, Vinik AI: Cigarette smoking and neuropathy in diabetic patients. Diabetes Care 1990; 13:434-437
- Edwards EA, Coffman JD: Cutaneous changes in peripheral vascular disease. Dermatology in General Medicine. New York, McGraw-Hill, 3rd Ed, 1987, pp 1997-2022
- Wright AL: Nails. BMJ 1988; 296:106-109
- Kontos HA: Vascular diseases of the limbs. Cecil's Textbook of Medicine. Philadelphia, WB Saunders Co, 18th Ed, 1988, pp 382-383
- Farish SE, El-Mofty SK, Cohn SJ: Intraoral manifestation of thromboangiitis obliterans (Buerger's disease). Oral Surg Oral Med Oral Pathol 1990; 69:223-226
- 0'Dell JR, Linder J, Markin RS, et al: Thromboangiitis obliterans (Buerger's disease) and smokeless tobacco. Arthritis Rheum 1987; 30:1054-1056
- Adar R, Papa MZ, Halpem Z, et al: Cellular sensitivity to collagen in thromboangiitis obliterans. N Engl J Med 1983; 308:1113-1116
- McLoughlin GA, Helsby CR, Evans CC, et al: Association of HLA-A9 and HLA-B5 with Buerger's disease. BMJ 1976; 2:1165-1166
- Herrick AL, Reiley F, Scholfield D, et al: Micronutrient antioxidant status in patients with primary Raynaud's phenomenom and systemic sclerosis. J Rheum 1994; 21:1477-1483
- Miller GH, Golish JA, Cox CE, et al: Women and lung cancer: a comparison of active and passive smokers with nonexposed nonsmokers. Cancer Detect Prevent 1994; 18:421-430
- Fontham ET, Canea P, Reynolds P, et al: Environmental tobacco smoke and lung cancer in nonsmoking women. a multicenter study. JAMA 1994; 271:1752-1759
- Willis RA: The Pathology of Tumors. London, Butterworth and Co, 1960, p 179
- Spencer PS, Helm TN: Skin metastases in cancer patients. Cutis 1987; 39:119-121
- Brownstein MH, Helwig EB: Metastatic tumors of the skin. Cancer 1972; 29:1298-1307
- Ihde DC: Paraneoplastic syndromes. Hosp Pract 1987; 22:105-124
- Omenn GS: Ectopic polypeptide hormone production by tumors. Ann Intern Med 1970; 72:136-138
- Jacobsen FK, Abildtrup N, Laursen SO, et al: Acrokeratosis paraneoplastica (Bazex syndrome). Arch Dermatol 1984; 120:502-504
- Kinlen LJ, Rogot E: Leukemia and smoking habits among United States veterans. BMJ 1988; 297:657-659
- Severson RK, Davis S, Heuser L, et al: Cigarette smoking and acute non-lymphocytic leukemia. Am J Epidemiol 1990; 132:418-422
- Miller K, Newell GR, Beeson WL, et al: History of cigarette smoking and risk of leukemia and myeloma: results from the Adventist Health Study. J Natl Cancer Inst 1990; 82:1832-1836
- Wald N: Smoking and leukemia. Am Cancer Soc J 1988; 13:4-5
- Hainsworth JD, Greco FA: Unrecognized leukemia cutis. Saudi Med J 1987; 80:663-664
- Leong CH: Cutaneous Clues to Systemic Diseases. Kent Ridge, Singapore University Press, 1986
- Horlick HP, Silvers DN, Knobler EH, et al: Acute myelomonocytic leukemia presenting as a benign-appearing cutaneous eruption. Arch Dermatol 1990; 126:653-656
- Cohen PR, Kurzrock R: Sweet's syndrome and malignancy. Am J Med 1987; 82:1220-1226
- Habboush HW, Lucie NP, Mackie RM, et al: Follicular mucinosis, mycosis fungoides, and acute myeloid leukemia. J Clin Pathol 1990; 43:347
- Spector JI, Zimbler H, DeLeo M, et al: Skin metastases from transitional cell bladder cancer. Urology 1987; 29:215-217
- Beautyman EJ, Garcia CJ, Sibulkin D, et al: Transitional cell bladder carcinoma metastatic to the skin. Arch Dermatol 1983; 119:705-707
- Flint GL, Flam M, Soter NA: Acquired ichthyosis. a sign of nonlymphoproliferative malignant disorders. Arch Dermatol 1975; 111:1446-1447
- Nicolis GD, Hetwig EB: Exfoliative dermatitis. Arch Dermatol 1973; 108:788
- Maurice TR: Carcinoma of the bronchus presenting with Henoch-Schonlein purpura. BMJ 1978; 2:831
- McLean DI, Haynes HA: Cutaneous aspects of internal malignant disease. Dermatology in General Medicine. New York, McGraw-Hill, 3rd Ed, 1987, pp 1917-1937
- Richardson JB, Callen JP: Dermatomyositis and malignancy. Med Clin North Am 1989; 73:1211-1220
- Cox NH, Lawrence CM, Langtry JAA, et al: Dermatomyositis. Arch Dermatol 1990; 126:61-65
- Basset-Sequin N, Roujeau JC, Gherardi R, et al: Prognostic factors and predictive signs of malignancy in adult dermatomyositis. Arch Dermatol 1990; 126:633-637
- Mills JA: Dermatomyositis. Dermatology in General Medicine. New York. McGraw-Hill, 3rd Ed, 1987, p 1835
- Newbold PCH: Skin markers of malignancy. Arch Dermatol 1970; 102:680-692
- Appell ML, Ward WQ, Tyring SK: Erythema gyratum repens: a cutaneous marker of malignancy. Cancer 1988; 62:548-550
- Ikeya T, Izumi A, Suzuki M: Acquired hypertrichosis lanuginosa. Dermatologica 1978; 156:274-282
- McLean DI, Macauley JC: Hypertrichosis lanuginosa acquisita associated with pancreatic carcinoma. Br J Dermatol 1977; 96:313
- Doll DC, McCagh MF, Welton WA: Sign of Leser Trelat. JAMA 1977; 238:236-237
- Karagas MR, Stukel TA, Greenberg ER, et al: Risk of subsequent basal cell carcinoma and squamous cell carcinoma of the skin among patients with skin cancer. JAMA 1992; 267:3305-3310
- Kabongo ML, Bedell AW: Nail signs of systemic conditions. Am Fam Physician 1987; 36:109-116
- Thomas PS, Sidhu B: Yellow nail syndrome and bronchial carcinoma. Chest 1987; 92:191
- Guin JD, Elleman JH: Yellow nail syndrome. Arch Dermatol 1979; 115:734-735
- Franks AG: Cutaneous aspects of cardiopulmonary disease. Dermatology in General Medicine. New York. McGraw-Hill, 3rd Ed, 1987, p 1988
- 0ksala E: Factors predisposing to oral yeast infections. Acta Odontol Scand 1990; 48:71-74
- Daling JR, Sherman KJ, Weiss NS: Risk factors for condyloma acuminatum in women. Sex Transm Dis 1986; 13:16-18
- Singer A, Walker PG, McCance DJ: Genital wart virus infection. nuisance or potentially lethal? BMJ 1984; 288:735-736
- Ferson M, Edwards A, Lind A, et al: Low natural killer-cell activity and immunoglobubin levels associated with smoking in human subjects. Int J Cancer 1979; 23:603-609
- Tollerand DJ, Clark JW, Morris B, et al: The effects of cigarette smoking on T-cell subsets. Clin Rev Respir Dis 1989; 139:1446-1451
- Clarke JR, Taylor IK, Fleming J, et al: The epidemiology of HIV-1 infection of the lung in AIDS patients. AIDS 1993; 7:555-560
- Neiman RB, Fleming J, Coker RJ, et al: The effect of cigarette smoking on the development of AIDS in HIV-1 seropositive individuals. AIDS 1993; 7:705-710
- Burns DN, Kramer A, Yellin F, et al: Cigarette smoking: a modifier of human immunodeficiency virus type 1 infection? J Acquir Immune Defic Syndr 1991; 4:76-83
- Christen AG, Swanson BZ, Glover ED, et al: Smokeless tobacco: the folklore and social history of snuffing, sneezing, dipping and chewing. J Am Dent Assoc 1982; 105:821-829
- Christen AG: The case against smokeless tobacco: five facts for the health professional to consider. J Am Dent Assoc 1980; 101:464-469
- US Department of Health and Human Services: The health consequences of using smokeless tobacco. A report of the Advisory Committee to the Surgeon General. NIH Publication No. 86-2874, 1986
- Squier CA: The nature of smokeless tobacco and patterns of use. CA Cancer J Clin 1988; 38:226-229
- Redmond DE Jr: Tobacco and cancer: the first clinical report, 1761. N Engl J Med 1970; 282:18-23
- Winn DM, Blot WJ, Shy CM: Snuff dipping and oral cancer among women in the southern United States. N Engl J Med 1981; 304:745-749
- Root HD, Aust JB, Sullivan A Jr: Snuff and cancer of the ear. report of a case. N Engl J Med 1960; 262:819-820
- Higginson J, Oettle AG: Cancer incidence in the Bantu and Cape colored races of South Africa: report of a cancer survey in the Transvaal. J Natl Cancer Inst 1960; 24:589-671
- Grady D, Greene J, Daniels TF, et al: Oral mucosal lesions found in smokeless tobacco users. J Am Dent Assoc 1990; 121:117-123
- Greer RO Jr, Poulson TC: Oral tissue alterations associated with the use of smokeless tobacco by teenagers. I. Clinical findings. Oral Surg 1983; 56:275-284
- Tyldesley WR: Tobacco chewing in English coalminers. malignant transformation in a tobacco-induced leukoplakia. Br J Oral Surg 1976; 14:93-94
- Roed-Peterson B, Pindborg JJ: A study of Danish snuff-induced oral leukoplakia. J Oral Pathol Med 1973; 2:301-313
- Offenbacher S, Weathers DR: Effects of smokeless tobacco on the periodontal, mucosal and caries status of adolescent males. J Oral Pathol 1985; 14:169-181
- Council on Scientific Affairs: Health effects of smokeless tobacco. JAMA 1986; 255:1038-1044
- Curry S, Edward HW, Grothaus LC: Intrinsic and extrinsic motivation for smoking cessation. J Consult Clin Psychol 1990; 58:310-316
- Silvis GL, Perry CL: Understanding and deterring tobacco use among adolescents. Pediatr Clin North Am 1987; 34:363-379
- Ockene JK: Physician-delivered interventions for smoking cessation: strategies for increasing effectiveness. Prev Med 1987; 7:723-737
- Peters JA: Nicotine-replacement therapy in cessation of smoking. Mayo Clin Proc 1990; 65:1619-1623